Charger Blogger Reflects on Experience in Emergency Medical Services
Beatrice Glaviano ’26 offers a peek into the life of a first responder, and she discusses what she’s learned about serving others while also taking care of herself.
April 4, 2024
By Beatrice Glaviano ’26
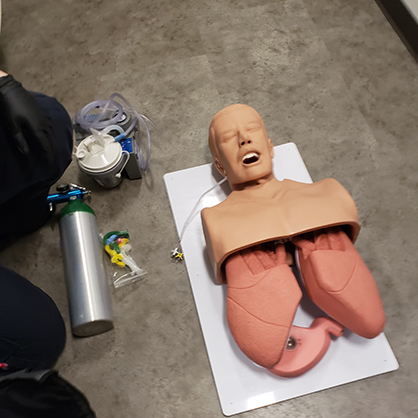
Beatrice Glaviano ’26 and her classmates have some fun training with 'Skelly.'
Author, once again sleep deprived: “Hello there, and welcome back.”
Dudes, this week has already been off to an interesting start, featuring:
I ran out of protein bars (so help me God)
Something is up with my hip, and yoga is not fixing it
I have to buy someone a birthday gift, and my original plan failed
As I am a woman, of course I’m overthinking possibly anything and everything about this thing
Help
I am working an overnight shift Thursday night, and it will be pouring
On a more serious note, though, eating-disorder recovery has kicked up a notch. With this, if my articles seem a bit more sparse, it’s not because I don’t love what I do. It’s simply because I may not have the emotional energy to go through them. Just thought I’d keep you guys in the ‘now’ with that, seeing that I prefer to be transparent with everyone here.
So: overnight shift. Let’s start with that.
As much as I’d like to be BFFs with a Tyrannosaur fossil who chases his own bone (Go fetch, Rexy!), this type of night shift involves a bit more than being a history buff.
Being an EMT student is interesting. Partially because a faculty member thought I had a doppelganger (EMT Beatrice vs. Nutritional Sciences Beatrice was something I found genuinely amusing), but also because it exposes you to the medical field in a very unique fashion.
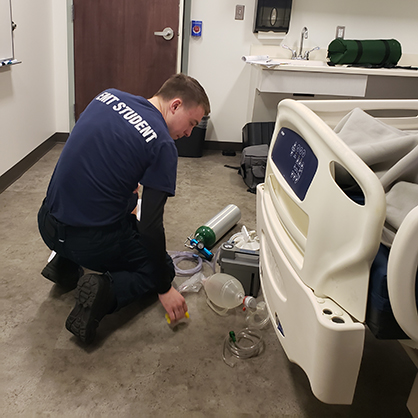
Beatrice Glaviano practices her EMS training.
Said fashion usually involves lights, sirens, Zofran, and Google Maps (no, I’m not kidding).
Anyhow, EMS – Emergency Medical Services – is a field that encompasses those who respond to situations in the prehospital setting. Some of the components that make up this field include dispatch centers, response units, healthcare facilities, EMS personnel (EMR, EMT, AEMT, Paramedic) and medical oversight. The main goal of EMS is to respond to emergency situations (i.e., 911 calls) of varying magnitudes as well as transport patients who are unable to travel without medical support on standby.
Yet, and I will say this, are all calls an emergency? No. Not all broken bones are emergencies, nor every shortness of breath. However, these situations have the capability to become emergent (something to always keep in mind), which is why EMS is called. We have the skills and training to potentially manage life-threatening circumstances, as well as the resources to give these patients further help down the line. Perhaps they need to be hospitalized, or they need a hug. We, as providers, are there for our patients in every moment that we are there with them.
Then there's gas station runs, talking with your paramedic about research because he’s like a podcast, eating a sandwich and dissociating after your first cardiac arrest (dissociation sandwiches do not taste like normal sandwiches, let me tell you), and the once again inevitable buzz of dispatch on the radio.
I remember the first time I heard that sound outside of the ambulance; the little ‘pow-pow-pow-pow’ signaling a 911. I don’t recall a time where I went from zero to one thousand percent adrenaline so quickly.
I got into EMS because a good friend of mine does it. He mentioned it, as it’s what he does for work and his career, and I found it to be curious. Obviously, at the time I had no clue how I’d do with it, seeing that I’d never done it ever in my life, nor did I have an innate curiosity toward it. But taking into the fact that I was a hospital child for a good chunk of my life, what was the harm in trying?
So, I registered for the classes here at UNewHaven. First semester is trauma, and the second is medical. Within that time period, you are learning about the many pathophysiologies of the human body and their presentation, the EMS system (government stuff, agh), and patient care, but also about yourself.
What type of provider do you want to be? How can you be better through the expectations you set for yourself? How do you deal with real-world situations?
Beatrice Glaviano ’26 observes while her classmates practice what they’ve learned.
Frankly, the best way to further yourself in any situation is research and the application of that newfound knowledge in the real world. As for the “real world,” it’s not the textbook. But, the textbook will give you your toolbox for you to put your tools (experiences) into. Trust me on that one. If you don’t know medical terms, anatomy/physiology, common drug types and names (i.e., aspirin, nitroglycerin, blood thinner names, common painkillers, conditions, etc.), uh...
I suggest Google and a re-evaluation of life choices. That’s all I will say. (Remember that it’s not only about you, but the patient. Poor or lack of knowledge will help neither of you).
Moving on into the real world, when you get your first ride time, you’re going to freak out a little bit. You’re going to pull up 100% freaking out internally, and almost forget to put your car in park. However, before you do this, set yourself up for success:
Bring a backpack with everything you could possibly need: snacks, water, laptop, homework, personal medical equipment (i.e., stethoscope), whatever. Make sure your backpack is relatively formal too; stick with neutral, basic colors (neon = your worst enemy).
Pack an extra pair of socks
Open mind, and a more open heart.
Uniforms are very big in EMS. Make sure yours is pristine; clean, ironed, and crisp. I highly suggest buying your own equipment even if your program may give you starter things. Getting myself a Littman Classic III was one of the best things I could do. Unlike double-tube stethoscopes, they offer a much higher quality of sound to the user and make your life a lot easier. Additionally, purchasing a personal pair of trauma shears and penlights isn’t a bad idea.
Alrighty. Now that you are a bit more equipment savvy and, presumably, have retained your lessons, now what?
Oh, right: ride time.
First day in, the first thing I was asked before we hopped aboard was:
“Is there anything you are uncomfortable with?”
“Uh, absolutely no clue.” This was the truth, given that I had done nothing else EMS related ever in my life. “Just throw me in, and I’ll let you know.”
One month later, I’m seeing something human but not human. Death jars you like that, I guess. What’s even more jarring is the fact that we’re advanced enough to undo death. With enough oxygen, CPR, an AED, and some epinephrine, you’ve got yourself a biological CTRL-Z.
An “undo” button, if you will.
They came back after being down for God-knows how long, though they died four hours later due to a brain bleed.
In EMS, we have some funky little weather patterns: white and black clouds. Personally, I’m a bit more of a gray one, but the two common ones are white and black. These indicate what calls you’ll get, or the shift you’ll have. White clouds? Easy calls, transfers, etc. This can be great, or super horrible. Black – as you’ve likely figured out – makes you a trauma magnet. Difficult patients? Yep. Need to call Fire for a lift assist? Also, yep. Oh, and it’s raining, and you forgot those extra socks.
Womp, womp.
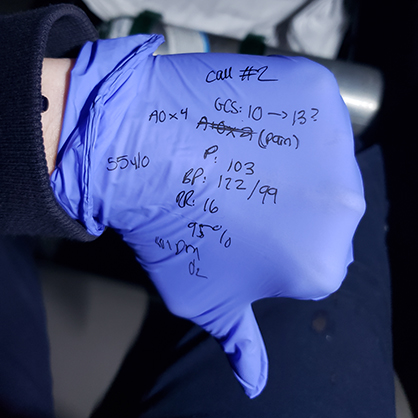
Beatrice Glaviano ’26 writes herself a few notes.
Being a gray cloud has enabled me to have a good mix of trauma, transfers, silence, and relatively good weather. Because I’ve only worked winter shifts, the worst thing that happened was finding my car half-frozen. Thank God.
I know that one day I’ll be hit with something nasty – it’s inescapable – but hopefully that will be at a time when I have enough experience and knowledge to back me up.
If this article has swayed any of you to perhaps even peek at the wide, wide world of EMS, I suggest asking Director Soto (of the UNewHaven Paramedicine Program) any questions that you may have when considering a career as an EMT or paramedic. Otherwise, nose around on the internet. There are a couple Facebook pages, Instagram and Twitter accounts on the world wide web that will definitely give you some different POVs to consider when potentially going into EMS.
However, the advice that I will give you comes down to one thing:
You are always the first patient.
EMS is draining. Sitting in an ambulance doing nothing is draining. Talking with patient after patient or dealing with high-stress situations is draining. I am going to 100% contradict myself when I say this, but you need to look after yourself first. If you cannot function, how on Earth are you supposed to provide adequate patient support?
With this in mind, I hope everyone is taking care of themselves this week and making sure to find balance between their academic, social, and health-based lives. Remember that if you are curious, be not afraid to ask some questions and get messy.
Take care everyone, and as always:
With peace, love, and peanut butter,
Beatrice